Maine Medical Center trained me well for dealing with orthopedic injuries. As residents we were lucky enough to train without orthopedic residents fighting over our broken bones, so I feel quite comfortable managing most acute fractures. But once the patient leaves the ER with their splint made with care and love, I'm not sure what the orthopedist's typically do from there. But here at KRCH I get to function as the ER doctor that treats the fracture acutely, and manages the patient in follow up. It's actually kind of nice, because for the most part, bones heal amazingly well, and it's been satisfying to see the patient in follow up, pain free. The following is just a smattering of some of the fractures I've seen during my time here at KRCH.
 |
Distal tibia and fibular fracture in a 24 year old male after falling off a roof. He was roofing and reportedly refused to wear the safety harness. I splinted him and subsequently casted him after attempting closed reduction, with some improvement in anatomic alignment. Unfortunately he did not return for his follow up appointment, so at this point some jungle doctor may have amputated his leg for all I know.
|
 |
| Supracondylar fracture in an 8 year old male. The patient was splinted in a posterior long arm splint and I casted him recently at his follow up appointment. We'll see him again in one month for reevaluation and likely cast removal. |
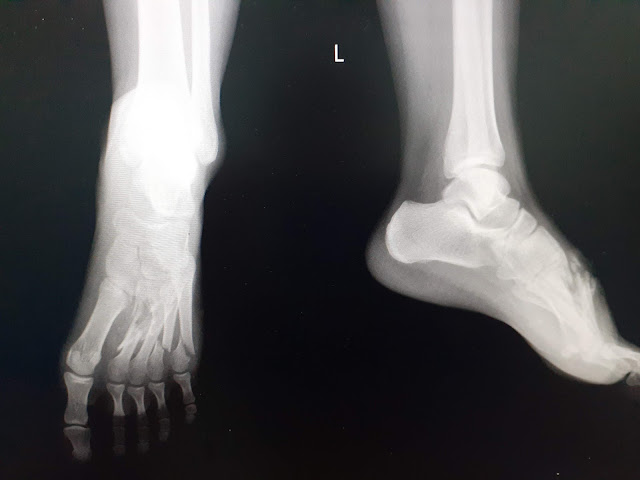 |
| Open fractures of the left 2nd through 5th metatarsals. |
 |
The above xrays are from a 14 year old girl who was one of two victims of a motorcycle accident. The other was an 18 year old girl who was unresponsive on arrival to the ER. I intubated her and she was emergently transported to Sanghkla Buri hospital. The above patient was in hysterics sitting in wheel chair in our tiny ER while we managed her unconscious friend. She suffered a distal radius fracture and a nasty left foot injury with multiple metatarsal fractures. I did a hematoma block for her wrist fracture and reduced and splinted her. She required sedation with ketamine for irrigation of her foot wound and subsequent splinting before also referring her for orthopedic management of her open foot fracture.
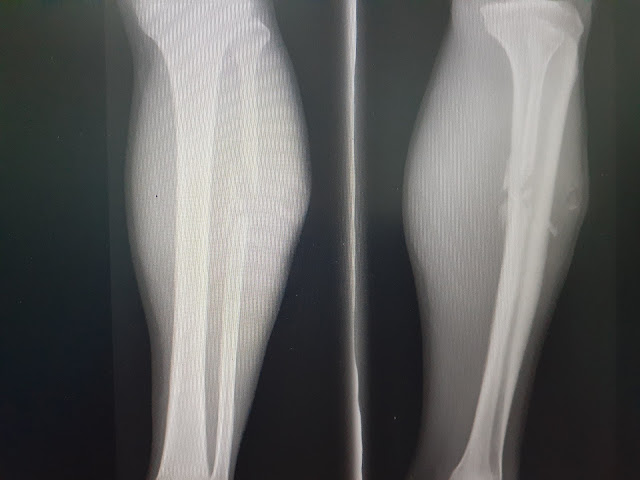 |
| Mid shaft fibular fracture in a Mon soldier after being involved in a skirmish with Burmese soldiers. He had no other injuries and only had this single bullet wound to his left calf. Dr. Jen irrigated the wound and placed a red rubber tubing catheter through the wound. Through this we were able to clean the wound daily until it had healed well. We placed him in a cast and he eventually was discharged back to the refugee camp on the Thai-Burmese border where he lived. |
|
 |
This is a pathologic femur fracture of a 74 year old male who was recently diagnosed with renal cell carcinoma. He is a lovely man who is a long time friend of the hospital. He reportedly had been having pain in his distal right thigh since June, so likely has metastases to his femur. He had a low level fall the night prior to presenting, and unfortunately fractured his right femur. We casted him and opted for conservative management. Fortunately we were able to transport him home to be with his family for the new year.
|
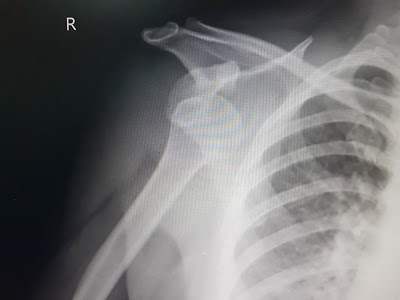 |
| Anterior shoulder dislocation after motorcylce accident in middle aged woman. She was in hysterics when she got to the ER and so I had to give her ketamine to get it back into place, which was easy once she was sedated. I saw her in follow up recently and she's back to cooking like crazy without any issues! |
 |
Right femoral neck fracture in an otherwise healthy 32 year old male sustained while playing soccer. The patient apparently was playing goalie and after jumping to stop a ball and landing directly on his right hip he was unable to walk for dayts. His xray showed a right femoral neck fracture. He was referred for likely surgical management.
|
This woman wasn't so lucky:
 |
This was an 80 year old female who came from the Safe house which is connected to KRCH with left hip pain after falling out of bed a few days earlier. She had significant pain with any movement of the hip. She held her leg in external rotation and had limb shortening. The above xray further supported the fact that she had an intertrochanteric left femur fracture. Unfortunately due to her age and other comorbidities we are opting for conservative management. I was able to treat her with a fascia iliaca block for pain control at least for one night and she went back to the safe house. Today I visited her at her home. She was sitting up in her bed, but still having difficulty sleeping. My hope is that by increasing her oral morphine she'll get some more relief. Unfortunately, she will be under strict bed rest for the next two months and will likely never walk again.

|















Comments
Post a Comment